Here’s something that surprises most people: growth hormone doesn’t stop mattering once you’re done growing. Not even close. Yet the conversation around it almost always circles back to height, kids, or athletes caught doping — and that’s a shame, because human growth hormone (HGH) is quietly one of the most important hormones your body produces across your entire lifespan.
Most of what the average American “knows” about growth hormone comes from headlines, supplement ads, or gym locker room conversations. And most of it is wrong, oversimplified, or actively misleading.
This guide is for anyone who wants the actual picture — the biology, the facts, the myths, and what it really means for your daily health. Whether you’re 25 or 65, this stuff is relevant to you.
What Is Growth Hormone and How Does It Work?
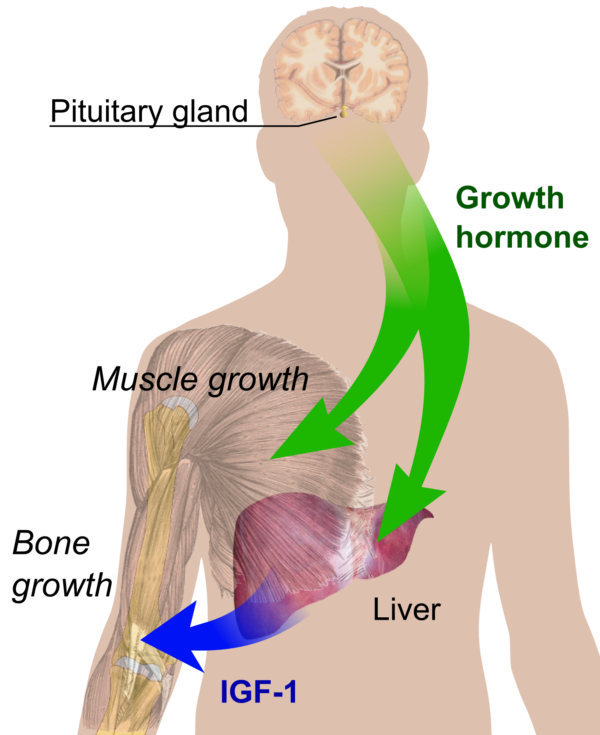
Growth hormone is a peptide hormone produced by your anterior pituitary gland — a pea-sized structure sitting at the base of your brain. It doesn’t act on tissues directly in most cases. Instead, it signals the liver to produce Insulin-like Growth Factor-1 (IGF-1), which then carries out much of the actual work: stimulating cell repair, protein synthesis, and tissue growth throughout the body.
Think of GH as the manager sending instructions, and IGF-1 as the team actually doing the job.
It travels through your bloodstream in pulses — short bursts rather than a steady stream. Most of those pulses happen at night, which is why sleep is so deeply connected to how well your body repairs itself. More on that in a moment.
One thing worth clearing up immediately: growth hormone is not a steroid. Anabolic steroids are synthetic versions of testosterone. GH is a completely different class of molecule with different mechanisms, different effects, and a different risk profile. Conflating the two is one of the most common misunderstandings out there.
Growth Hormone Does Much More Than Increase Height
This is where most people’s mental model breaks down. By adulthood, the growth plates in your bones have closed — so HGH is no longer adding inches to your frame. But it’s still doing a lot.
In adults, growth hormone plays a real role in:
- Bone density — It supports ongoing bone remodeling, which matters a lot for osteoporosis risk as you age.
- Lean muscle mass — GH promotes muscle recovery and helps maintain the muscle-to-fat ratio in your body.
- Fat metabolism — It signals adipose tissue (body fat, especially visceral fat) to break down for energy. This is partly why low GH levels in adults are associated with increased belly fat.
- Collagen production — Your skin, tendons, and connective tissue rely on collagen. GH contributes to its production, which is one reason GH decline is associated with changes in skin elasticity.
- Organ maintenance — Several organs, including the heart and kidneys, depend on adequate GH signaling to function optimally over time.
So when GH levels drop — which they naturally do with age — the downstream effects are scattered across your whole body. It’s not dramatic, it’s gradual. But it’s real.
Sleep Is the Biggest Natural Trigger for Growth Hormone
If there’s one lifestyle factor that most directly controls your GH output, it’s sleep. Specifically, deep sleep — what researchers call slow-wave sleep — is when the pituitary gland releases the largest hormone pulse of the day.
Your body is built around a circadian rhythm, and GH release follows it tightly. Most of that release happens in the first few hours of the night, during the deepest stage of your sleep cycle. Melatonin, which rises as daylight fades, helps set that biological clock.
When you cut sleep short, stay up late, or sleep poorly, you don’t just feel groggy the next day. You genuinely suppress that hormone pulse. Over time, chronic sleep deprivation is one of the most reliable ways to tank your body’s natural GH production — and the research on this is pretty consistent.
This is also why athletes who prioritize sleep recovery aren’t just being precious about their routines. The biology backs them up completely.
Exercise Stimulates Growth Hormone — But Not All Workouts Are Equal
Exercise is one of the most powerful natural stimulators of GH release, but the type of exercise matters a lot more than most people realize.
Here’s a rough breakdown of how different training approaches compare:
| Training Type | GH Stimulation | Notes |
|---|---|---|
| High-Intensity Interval Training (HIIT) | Very high | Short bursts push lactate threshold, a key GH trigger |
| Heavy resistance training | High | Compound lifts especially effective |
| Moderate steady-state cardio | Moderate | Useful, but less potent than intensity-based work |
| Light walking or stretching | Low | Still beneficial for overall health, minimal GH effect |
In my view, the HIIT finding is the most underappreciated. The mechanism seems to involve lactate accumulation — when your muscles produce lactate during intense effort, it appears to signal the pituitary to release more GH. This doesn’t mean you need to destroy yourself every session, but it does suggest that some level of intensity matters.
Recovery matters too. Overtraining can actually backfire by chronically elevating cortisol, which suppresses GH. So the pattern of pushing hard, then recovering well, is what actually optimizes hormone output over time — not just grinding through workouts regardless of how you feel.
Nutrition Influences Growth Hormone More Than Most People Realize
What you eat — and when you eat — shapes your GH levels more directly than most diet advice acknowledges.
The most important factor is insulin. When blood sugar rises sharply (after a high-carb or sugary meal), insulin spikes, and elevated insulin suppresses GH release. This is why the timing of meals relative to exercise and sleep matters.
Protein intake is genuinely important. Certain amino acids — particularly arginine and glutamine — have been shown in research to support GH secretion. Getting enough dietary protein from whole food sources gives your pituitary what it needs to do its job.
Intermittent fasting has attracted real scientific interest here. When you extend the overnight fasting window — say, skipping breakfast or eating within an 8-hour window — insulin levels stay lower for longer, and GH pulses tend to be more pronounced. The research isn’t settled enough to make sweeping claims, but the pattern is consistent enough to be worth knowing about.
Added sugar is probably the biggest dietary obstacle for most Americans. Regular consumption of high-sugar foods chronically elevates insulin, which chronically blunts GH release. It’s a slow erosion, not a dramatic drop-off — but over years, it adds up.
Common Myths About Human Growth Hormone
A few of these myths are worth calling out directly.
“HGH is a fountain of youth.” It isn’t. GH levels do decline with age — roughly 1-2% per year after your 30s — but supplementing with exogenous HGH in healthy adults hasn’t been shown to reliably reverse aging. Some studies have noted modest changes in body composition, but also side effects like joint pain, fluid retention, and increased cancer risk with higher doses.
“More GH is always better.” This is flat wrong. Excess GH leads to a condition called acromegaly — abnormal bone and organ growth, cardiovascular problems, and shortened lifespan. The body maintains tight regulation of GH for good reason.
“Supplements can significantly raise your HGH levels.” Most “HGH boosters” sold online are either amino acid blends with modest effects, or completely ineffective. The FDA doesn’t approve them for HGH deficiency. Prescription HGH is an injectable medication — pills and powders claiming to raise HGH meaningfully should be viewed skeptically.
The internet is full of celebrity-endorsed anti-aging claims about GH. Apply your usual skepticism.
Who Actually Needs Growth Hormone Therapy?
Legitimate GH therapy exists and genuinely helps people — but it’s for a narrow medical population, not healthy adults looking for an edge.
Diagnosed growth hormone deficiency (GHD) can occur in children (affecting growth and development) and adults (affecting metabolism, bone density, and quality of life). An endocrinologist diagnoses it through IGF-1 blood tests, and sometimes MRI imaging of the pituitary gland.
Conditions that may warrant GH therapy include childhood GHD, Turner syndrome, chronic kidney disease in children, and adult GHD following pituitary damage or surgery. In these cases, prescription HGH therapy is carefully monitored and can be genuinely life-changing.
What it isn’t: an appropriate treatment for healthy adults who want to lose weight, build muscle, or slow aging. Using GH outside of a diagnosed deficiency isn’t just legally murky in the U.S. — it carries real health risks.
Little-Known Facts About Growth Hormone That May Surprise You
A few things that tend to surprise people when they learn them:
GH decline is normal and gradual. Levels peak in adolescence and drop steadily from your late 20s onward. This isn’t a medical problem for most people — it’s biology.
Men and women produce GH differently. Women generally have more frequent GH pulses throughout the day, while men tend to have larger single pulses, especially during sleep. Estrogen appears to increase GH secretion, which is one reason menopause can affect body composition in ways that aren’t purely about estrogen itself.
Chronic stress is a direct suppressor. Elevated cortisol — your main stress hormone — inhibits GH release. This is one of the more underappreciated connections between stress management and physical health.
Body fat percentage matters. Higher levels of visceral body fat are associated with reduced GH secretion, creating a cycle: low GH leads to fat accumulation, and excess fat further suppresses GH. Losing weight, particularly abdominal fat, tends to improve natural GH output.
Lifestyle changes can meaningfully improve your natural levels. This is actually good news. You don’t need a prescription to meaningfully support your GH. Sleep, intensity-based exercise, appropriate nutrition, stress management, and maintaining a healthy weight are — together — genuinely effective levers.
Frequently Asked Questions
Can adults naturally increase growth hormone?
Yes, meaningfully so. Prioritizing deep sleep, incorporating high-intensity exercise, managing blood sugar through diet, maintaining a healthy weight, and reducing chronic stress all support natural GH production. These aren’t magic fixes — but the research supporting their effect is solid.
Is growth hormone legal in the United States?
Prescription HGH is legal when prescribed by a licensed physician for an FDA-approved medical condition. Using it without a prescription, or using it for off-label purposes like anti-aging or athletic performance, is not legally sanctioned and carries potential health risks.
Does growth hormone help with weight loss?
GH does play a role in fat metabolism, particularly for visceral fat. In people with diagnosed GHD, hormone therapy often improves body composition. In healthy adults without a deficiency, the evidence for weight loss specifically is much weaker — and the risks of unsupervised use are real.
Can diet alone increase HGH?
Diet can support or undermine your natural GH production, but it’s unlikely to dramatically raise levels on its own. Reducing added sugar, getting adequate protein, and experimenting with intermittent fasting can all help. Think of diet as one piece of a larger lifestyle picture.
Is growth hormone safe without a prescription?
No. Injectable HGH without medical oversight carries significant risks, including joint pain, insulin resistance, edema, and long-term concerns about cancer and cardiovascular health. The over-the-counter “boosters” aren’t the same thing — they’re mostly ineffective rather than dangerous — but they’re also not worth your money.
Key Takeaways
Growth hormone affects far more than how tall you grew. It’s a central player in metabolism, body composition, bone health, and recovery throughout your adult life.
The most reliable ways to support it don’t require a prescription: get quality sleep, exercise with some intensity, eat enough protein, manage your blood sugar, and don’t let chronic stress become the background noise of your life.
Prescription GH therapy is genuinely helpful — for people who actually need it, diagnosed by a real endocrinologist, and monitored carefully. It’s not a shortcut for everyone else.
Most of the supplement industry’s messaging around HGH is marketing, not medicine. That gap between what’s sold and what’s proven is where a lot of people get misled.
And when in doubt, the right person to talk to about your hormone health isn’t a wellness influencer — it’s a qualified healthcare professional who can actually test what’s happening in your body.

Jay Lauer is a health researcher with 15+ years specializing in bone development and growth nutrition. He holds a B.S. in Kinesiology and is a certified health coach (ACE). As lead author at HowToGrowTaller.com, Jay has published 300+ evidence-based articles, citing sources from PubMed and NIH. He regularly reviews and updates content to reflect the latest clinical research.